In Mississippi, where the abortion case ended Roe v. Wade before the Supreme Court, Governor Tate Reeves vowed that the state would now “take all necessary steps to support mothers and children. “
Today, however, Mississippi is underperforming on any of these goals. The infant and maternal mortality rates here are among the worst in the nation.
State leaders have rejected the Affordable Care Act’s Medicaid expansion, leaving estimates alone 43,000 women of childbearing age no health insurance. They chose not to extend Medicaid to women for a year after giving birth. And they have a welfare program that offers some of the country’s least generous cash aid – the max $260 a month for a poor mother raising two children.
Mississippi embodies a national stereotype: States that ban abortion, or are expected to have the nation’s weakest social services for women and children, and have child mortality rates infants and mothers are taller.
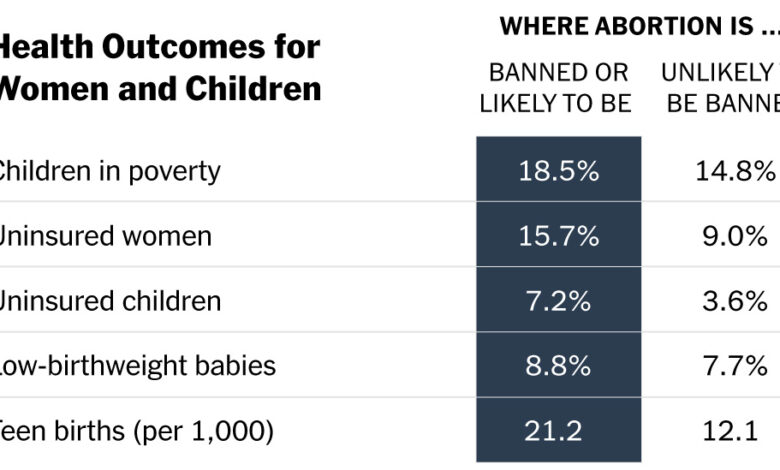
According to analysis by the New York Times, the 24 states that have banned abortion (or likely will) have worse outcomes on a variety of outcomes than states where abortion will likely remain legal, including the rate of abortion. child and maternal mortality, adolescent birth rate and uninsured percentage of women and children. States that have the ability to ban abortion or have laws before Roe ban abortion; recently passed strict restrictions; or have legislatures actively considering new bans.
The majority of these states have refused to extend Medicaid’s year-long extension after birth. Nine people rejected the Affordable Care Act’s Medicaid expansion, which provides health care to the poor. No one is asking new parents to take paid time off work to care for their newborn.
Carol Burnett, who works with single and poor mothers as the CEO of Mississippi Low Income Childcare Initiative, a non-profit organization. “All of these proven state-level obstacles prevent mothers from getting the help they need, the health care they need, the childcare they need.”
Many anti-abortion activists have acknowledged that improving the health and livelihoods of mothers and children is an important goal for their movement: “This is my lecture to the pro-life movement. life last year,” said president Kristan Hawkins. of the Student for life. “No woman stands alone in post-Roe America.”
Social spending is not the only answer to poverty and poor public health, and some in the anti-abortion movement insist they want to help women and children – not with more government spending. But there is a strong link between state policy choices and outcomes for mothers and children, researchers have found.
Perhaps the most obvious example is health insurance. Much learn tied it to improving the health and financial security of poor Americans. Since 2014, states have had the option expand their Medicaid programs to cover nearly all poor adults, with the federal government paying 90 percent or more of the cost. But nine of the states that plan to ban abortion have not expanded it, citing oppose Obamacare, which Republicans have long vowed to repeal; don’t want to provide health benefits to poor Americans who doesn’t work?; or concerned about 10 percent of the bill left to state governments to fund.
“Narrowing the Medicaid gap is the first and best choice for women’s health care,” said Allison Orris, a senior fellow focusing on health policy at the Center for Budget and Policy Priorities. to the left.
As of 2021, states also have the option to expand Medicaid to cover women within a year of giving birth instead of two months. Only 16 states have refused to do so or opted for a shorter time – all but three are also banning or seeking to ban abortion.
Poor and pregnant women are eligible for Medicaid nationally, and the program pays for 4/10 births nationwide. However, health experts say it is important for women to be covered for a long time after giving birth and in the years before becoming pregnant. Conditions such as diabetes, cardiovascular disease, and substance abuse can lead to pregnancy complications and poor newborn health. Research shows that Medicaid expansion can reduce maternal mortality. Medicaid also pays for contraceptives.
Another example is paid family leave and subsidized childcare. No state prohibits abortion (or is likely to) guarantee parents paid leave to care for and bond with their newborn. Only 11 states and the District of Columbia do. Paid leave has been shown for healthy for babies and mothers’ mental and physical health as well as theirs economic outlook.
In most states, there is no guaranteed childcare for children until they enter kindergarten at age 5. Subsidies for low-income families spread a small segment eligible children, different, from less than 4 percent in Arkansas (currently banning abortion) to more than 17 percent in Vermont (where abortion rights legislation has been passed).
In many states, benefits also raise a conundrum: Parents have to work to get them, but they can’t find or start work without a caregiver. Some states add other obstacles. Mississippi requires single mothers to apply for child support from the father before they can receive benefits. Also, a job that pays minimum wage — no higher than the federal floor of $7.25 in 20 states — doesn’t necessarily pay enough to cover even subsidized care.
Support for families is different in some states when the child is 3 or 4 years old. Thirteen states and the District of Columbia provide or have committed to providing universal preschool. Unlike other family benefits, the anti-abortion states are nearly as capable of providing public preschool. Six of the 13 states ban abortion or may.
“This is consistent with the view that education is a public responsibility, while other safety net programs are not,” said Steven Barnett, senior co-director of the National Institute of Early Education Research at Rutgers. “is beyond the scope of public responsibility accepted in conservative countries. “
Poorer states may have fewer resources to fund benefits such as parental leave, or additional state for the federal earned income tax credit. Zachary Parolin, a professor of social policy at Bocconi University in Milan, who has studied how states use the broad discretionary power that the Temporary Assistance program for impoverished families grants them. may be disclosed.
“You can’t say that Alabama gives very little cash to low-income families with children because they can’t afford it,” Parolin said. “It has a TANF program, and it is primarily funded by the federal government.”
But in 2020, Alabama just spent about 8 percent of its welfare fund on direct cash assistance to families. Mississippi spent 5 percent. Instead, states typically spend these subsidies on a variety of other programs such as premarital advertising campaigns and abstinence-only sex education (in 2020, a state auditor in Mississippi) found out that states miss out on millions of dollars in federal benefitsincluding speeches never delivered by Former midfielder Brett Favre).
Mr. Parolin’s research has shown that states have a larger proportion of Black populations tend to spend the least on cash support, widening the poverty gap in America between black and white children. Similarly, the Times analysis also shows that states likely to ban abortion will spend a smaller portion of welfare funds on basic support.
Countries with less generous safety net programs also often use complicated rules and paperwork arrive further restrict access to benefitsSarah Bruch, professor of social policy and sociology at the University of Delaware. The United States can help women and families, she said, not only by investing more in the safety net, but also by making it easier to find and use.
Angela Rachidi, a senior research fellow in poverty and safety net programs at the right-leaning American Enterprise Institute, says government has several roles but it’s not alone: has a broader responsibility as a society – employers, churches, organizing communities – to make sure mothers feel they can bring those kids into the world. “
The evidence to date suggests that such organizations will struggle to meet the growing demand.
Following the Supreme Court decision, other governors banning abortion have announced their commitment to pregnant women and children. J. Kevin Stitt, governor of Oklahoma, wrote in a executive order signed on 11 July.
Oklahoma ranks among the 10 worst states in terms of child poverty, infant mortality and the percentage of women of childbearing age without health insurance.
In Texas on the day of the ruling, Governor Greg Abbott said in a statement that the state has “prioritised supporting the health care of women and mothers-to-be in need.” On Wednesday, the governor’s press secretary, Renae Eze, said, “We look forward to continuing to work with the Legislature to ensure the health of all Texas women and their families.”
Mr. Abbott pointed to Texas’ decision to provide mothers with Medicaid coverage six months after giving birth. The state declined the full year coverage offered by the federal government. Texas has also used techniques to remove children from Medicaid coverage for invalid documents. It has a higher proportion of uninsured children and women of reproductive age than any other state.
In legislation restricting abortion, Texas has earmarked $100 million over two years for a program that connects women with counseling, education, and provision, called Alternatives to Abortion. That funding pales in comparison to another benefit, which Texas has denied – estimated $6 billion in federal funds each year that it is losing by choosing not to expand Medicaid.
Josh Katz contribution report.
Summary:
Source: Poverty Data (2019) from the American Community Survey; non-insurance data (2019) from ACS; low birth weight data (2019) from the Centers for Disease Control and Prevention; adolescent birth data (2019) from CDC; maternal mortality data (2018-20) from CDC; infant mortality data (2018-19) from CDC; Medicaid Extended Data (2022) from the Kaiser Family Foundation; paid leave data (2022) from the National Partnership for Women and Families; preschool data (2022) from the National Institute of Early Education; minimum wage data (2022) from the Department of Labor.
Results table: Maternal mortality data (2018-20) from CDC; infant mortality data (2018-2019) from CDC; poverty data from ACS (2019); non-coverage data from ACS (2019).
Policy Table: Extended Medicaid Data (2022) from the Kaiser Family Foundation; paid leave data (2022) from the National Partnership for Women and Families; preschool data (2022) from the National Institute of Early Education; minimum wage data (2022) from the Department of Labor.




